INTRODUCTION
Gout is a medical condition that usually presents with recurrent attacks of acute inflammatory arthritis (red, tender, hot, swollen joint). It is caused by elevated levels of uric acid in the blood. The uric acid crystallizes and deposits in joints, tendons, and surrounding tissues. Gout affects 1% of Western populations at some point in their lives.Treatment with NSAIDs, steroids, or colchicine improves symptoms. Once the acute attack has subsided, levels of uric acid are usually lowered via lifestyle changes and long term prevention with allopurinol Historically, it was known as "the disease of kings"or "rich man's disease".
Signs and symptoms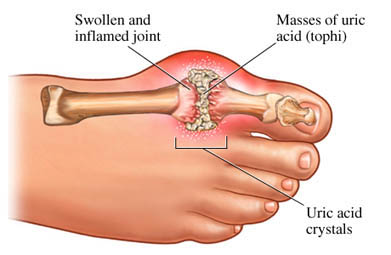
Tophi of the knee.
Gout usually presents as recurrent attacks of acute inflammatory arthritis (a red, tender, hot, swollen joint). The joint that is most commonly affected is the first
metatarsalphalangeal joint at the base of the big toe (approximately 75 percent of first attacks) and when this occurs it is known as podagra. The reason gout usually presents in the feet is in part due to the lower temperature.People with long-standing hyperuricemia can form tophi (uric acid crystal deposits) in tissues. These are usually hard, non-painful deposits. Extensive tophi that invade bone are associated with arthritis due to bone erosion.Elevated levels of urine uric acid can lead to uric-acid crystals precipitating in the kidneys which may form kidney stones and lead to urate nephropathy.
Causes
Hyperuricemia is the underlying cause of gout. This can occur for a number of reasons including dietary, genetic, or underexcretion of urate.[1] About 10% of people with hyperuricemia develop gout.
Medical conditions
Gout may present as a complication of other medical conditions.
• Metabolic syndrome (the combination of hypertension, diabetes, dyslipidemia,
truncal obesity, increased cardiovascular disease risk)
• Leukemia
Gout also can develop as a co-morbidity of other diseases, including polycythaemia, intake of cytotoxics, obesity, diabetes, hypertension, renal disorders, and hemolytic anemia. Gout is an important complication in a minority of solid organ transplants.Gout may occur as a result of renal failure.[ An example of this is a condition known as Chronic Urate Nephropathy in which crystal deposits form in the renal tubules,interstitium and glomeruli. This results in elevated serum creatinine, urinary sediments,and hyperuricemia disproportionate to the degree of renal insufficiency. Renal impairment is common in patients with gout but usually occurs secondary to other conditions.
Some studies have established a statistical connection between gout and lead poisoning,and a significant correlation between levels of lead in the body, urate excretion and gout.It is known that lead sugar was formerly used to sweeten wine. This condition is then known as saturnine gout, as saturnus is the alchemical term for metallic lead.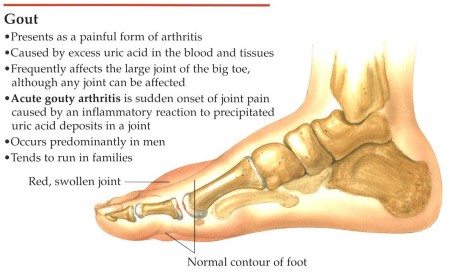
Pharmaceuticals
Diuretics have been associated with attacks of gout; low doses of hydrochlorothiazide (HCTZ), however, do not seem to increase the risk.
Pathophysiology
Gout occurs when crystals of uric acid, in the form of monosodium urate, precipitate on the articular cartilage of joints, on tendons, and in the surrounding tissues. Uric acid is a normal component of blood serum. Uric acid is more likely to form into crystals when there is hyperuricemia, although hyperuricemia is 10 times more common without clinical gout than with it.Gout can also occur when serum uric acid is normal, and when it is abnormally low (hypouricemia). Paradoxically, acute attacks of gout can occur together with a sudden decrease in serum uric acid, such as due to use of drugs (uricosurics, xanthine oxidase inhibitors), or total parenteral nutrition. However, the sudden decrease may be a consequence of abrupt formation of crystals (removing uric
acid from the serum), rather than a cause.Regardless of the serum concentration of uric acid, precipitation of uric acid is markedly enhanced when the blood pH is low (acidosis). A similar pH-sensitive effect occurs in urine, contributing to uric acid nephrolithiasis (kidney stones).Uric acid is a product of purine metabolism, and in humans is normally excreted in the urine. Purines are generated by the body via breakdown of cells in normal cellular turnover, and also are ingested as part of a normal diet. The kidneys are responsible for approximately two-thirds of uric acid excretion, with the liver responsible for the rest.
Diagnosis
Spiked rods of uric acid (MSU) crystals photographed under a microscope with polarized light from a synovial fluid sample. Formation of uric acid crystals in the joints are associated with gout.
Synovial fluid
A definitive diagnosis of gout is based upon the identification of monosodium urate
(MSU) crystals in the synovial fluid. They have a needle-like morphology and strong
negative birefringence under polarized light. This test is difficult to perform and often
requires a trained observer.
Blood tests
Hyperuricemia is a common feature of gout, so its presence supports a diagnosis of gout.
However, gout can occur without hyperuricemia.[24] Hyperuricemia is defined as a
plasma urate (uric acid) level greater than 420 μmol/L (7.0 mg/dL) in males, or 380
μmol/L in females. However, a high uric acid level does not necessarily mean a person will
develop gout. Urate is within the normal range in up to two-thirds of cases.[25] If gout
was suspected, the serum urate test should be repeated once the attack has subsided.
Other blood tests commonly performed are full blood count, electrolytes, renal function,
thyroid function tests and erythrocyte sedimentation rate (ESR). This helps to exclude
other causes of arthritis, most notably septic arthritis, and to investigate any underlying
cause for the hyperuricaemia.
Differential
A critical differential diagnosis in gout is septic arthritis. The only way to definitively
rule out this diagnosis is via a joint aspiration and culture.
Clinically, gout can be hard to distinguish from several other conditions, including
chondrocalcinosis. Chondrocalcinosis is a very similar disease, caused by deposition of
calcium pyrophosphate rather than uric acid.
Gouty tophi, particularly when not located in a joint, can be mistaken for basal cell
carcinoma or other neoplasm.